
By: Dr. Musa Marenah
Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition. The health of all peoples is fundamental to the attainment of peace and security and is dependent on the fullest co-operation of individuals and States.
The achievement of any State in the promotion and protection of health is of value to all. Unequal development in different countries in the promotion of health and control of diseases, especially communicable disease, is a common danger. Healthy development of the child is of basic importance; the ability to live harmoniously in a changing total environment is essential to such development. The extension to all peoples of the benefits of medical, psychological and related knowledge is essential to the fullest attainment of health. Informed opinion and active co-operation on the part of the public are of the utmost importance in the improvement of the health of the people. Governments have a responsibility for the health of their peoples which can be fulfilled only by the provision of adequate health and social measures.
sexual health as a state of physical, emotional, mental and social well-being related to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all individuals must be respected, protected and fulfilled.
normal structure of female external genitalia has labia majora ie the big lip which closes the external genital. labia minor ie the minor lip which is underneath the labia majora,
clitoris which is a penile like structure above the two labia. the exposed tip of the clitoris which is the part seen in most women is called the glan. The clitoris and its glan has a covering called the clitoris hood also called the prepuce of the clitoris.
there are three opening into the vulva ie the urethra also calls the urinary opening. There are other glans around the urethra calls the skene glans. The vagina is where menstrual blood and baby passes through as well as natural coitus happen and two Bartholin glan ducts or openings which produces secretions.
CIRCUMCISION is the procedure that involves removal of the foreskin or prepuce or redundant skin over the glans. Either penis or clitoris.
MUTILATION OR MAIMING (from the Latin: mutilus) is severe damage to the body that has a subsequent utterly ruinous effect on an individual’s quality of life.
In the modern era, the term has an overwhelmingly negative connotation, referring to alterations that render something inferior, dysfunctional, imperfect, or ugly.
From the above definitions: theoretically as well as in practice there is a difference between circumcision and genital mutilations.
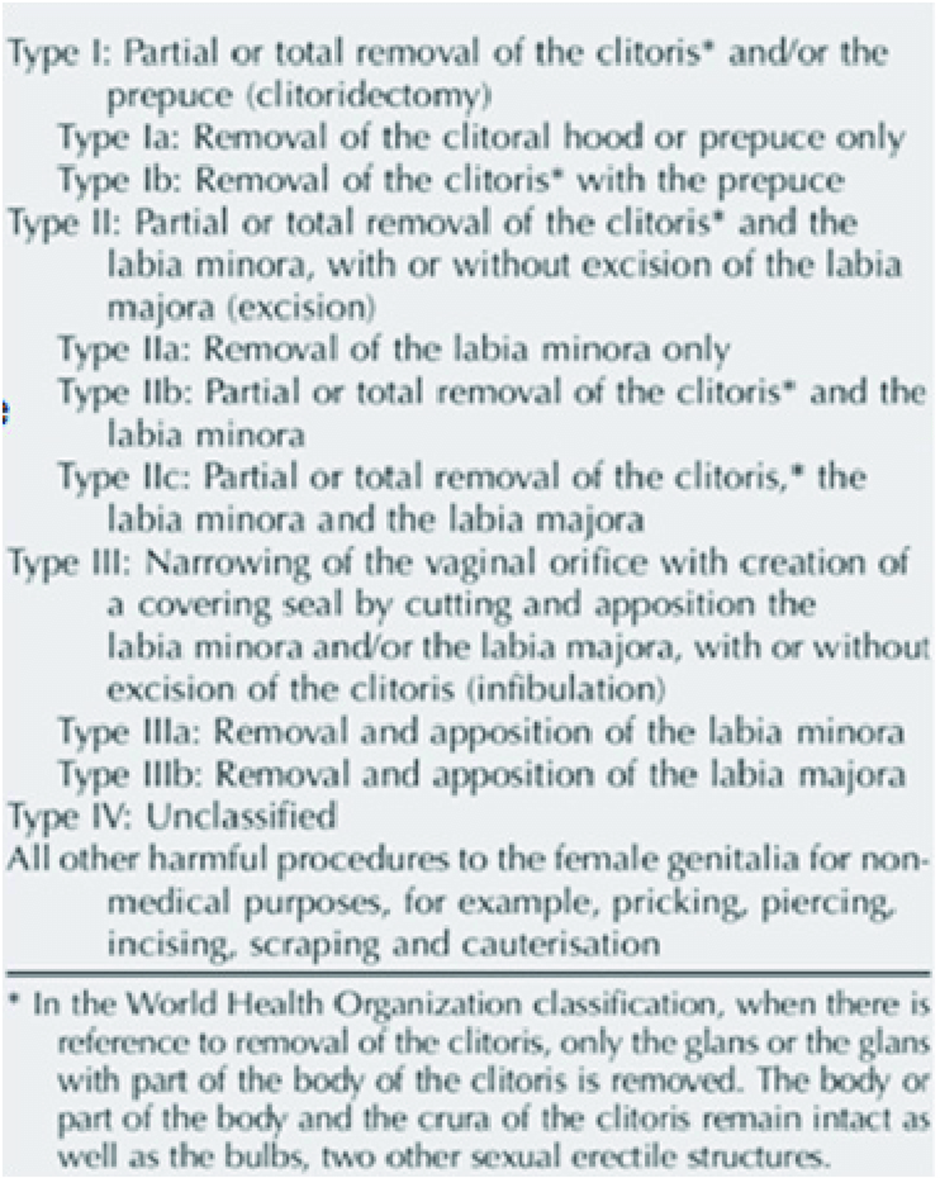
WHO classification of FGM/C
An estimated 200million girls and women worldwide have been subjected to this practice.
Reasons given for the practice of FGM/C are based on cultural and religious beliefs and some types have no basis in science.
FGM/C is a deep-rooted practice mostly conducted on women and girls by elderly women designated to carry out this practice in the community. It may involves cutting the prepuce (clitoral hood), clitoris, labia minora and/ or in some extensive form part of the labia majora is removed and sealed. The trade is inherited through culture, tradition and family linage. The act varies depending on the ethnic group and geographical location. The instruments used to carry out the circumcision is mostly ceremonial knives that has been passed on to generations, scissors, razors or pieces of glass and some instances fingernails are used to conduct it on babies. These instruments are frequently re-use without been sterilized. With advanced in medicine, sometimes its performed by healthcare workers with medical instruments and under sterile conditions.
In addition to the unhygienic ways in which the circumcision has been carried out, the concoction applied to the wound can be made from different substances that are not sterile such as ashes, porridge, herbs, cow dung and lime juice.
In The Gambia
Female circumcision is one of the oldest “operative” procedures in the Gambia others include tribal markings, tattooing of lips and gum etc. Its mainly done for traditional requirement or for religions obligation. In the past its usually done to children just before puberty as a right to passage from childhood to adolescence and adulthood.
Recently children as young as neonates have undergone the procedure. The procedure is performed by a wide range of practitioners from traditional practitioners’ call ‘ngansinba” to health care providers doctors and nurses. This has led to various types of Female genital mutilation or cutting in the country. The commonest type is type 1 type 2. Type 3 and type 4 are rare. Type 4 is also common among educated/affluent and those who have travelled overseas.
A 2010 survey in The Gambia among women of reproductive age put the prevalence rate of FGM/C at 76.3%. FGM/C was banned in 2015, but there is no real effort at enforcement of the ban. This study aimed to provide national data on obstetric outcomes to support advocacy and health education. A multicentre observational study to assess the obstetric and neonatal outcomes of parturient women with and without FGM/C was carried out across 4 healthcare facilities in The Gambia. The primary outcome was postpartum haemorrhage (>500ml) and secondary outcomes were caesarean section, perineal tears (including episiotomy), neonatal resuscitation and perinatal death. Of the 1,569 participants recruited into the study, 23% had no FGM/C while 77% had FGM/C of varying severity. The risk of postpartum haemorrhage was doubled for women with type I FGM/C, tripled in type II FGM/C and increased by 5-fold for those with type III and IV FGM/C. Caesarean section and perineal tears were also increased. FGM/C was associated with increased risk for neonatal resuscitation and perinatal death. FGM/C is associated with poor obstetric and neonatal outcomes in the Gambia with degree of risk correlating with the severity of FGM/C. Idoko et al
About the study despite finding, have limitations and contradicted the theory that complications are proportional to the amount and degree of the excision ie type 1 has lesser complications than type 2
A range of cutting instrument are use from razor blades to scalpel which many or may not be sterile in variety of conditions from bush, homes to health facilities.
The advocation on the consequences of female genital cutting on health have been around since 1980s. A lots of achievements have been made since the beginning of the advocacy despite all these advocacies almost all studies focus on the prevalences as very high there is no study done on the incidence which will show the impact of the advocacy over the years. With very few studies assessing the various types and subtypes.
Gambia Demography health Survey 2019/2020 shows
Women who believe FGM/C should continue decreased from 65% in 2013 to 46% in 2019-20. This decrease was largest among women who have undergone FGM/C. According to the 2019-20 Gambia Demographic and Health Survey (GDHS), nearly 5 in 10 girls age 0-14 in The Gambia have undergone FGM/C. More than 6 in 10 women who have undergone FGM/C were cut before age 5. FGM/C ranges from 25% of girls in Banjul to 79% of girls in Basse.
The crossroad came recently
The 1996 constitution has gone through at least 52 amendments during the 22yrs. Most people have considered that period as a dictatorship hence all laws including amendments were not for greater good but for the benefit of the dictatorship, since the change of government many laws have been amended. This act should not be an exception.
On the 17th December 2015 which the women act 2010 was amended to include Female circumcision. Since the ascending to the law no one was charged or convicted. There is no records that wide consultation was made prior to passage of 2015 bill including record that ministry of health was consulted, had made any contribution or send a position paper before the law was enacted.
In august 2023 when three women from Niani Bakadagi Mandinka where trial, convicted and fine for female circumcision. This conviction has been a huge set back to the gains made and had revive the counter narrative on Female Genital cutting
Various publications states some of the consequences of female genital cutting FGC if it is done unsafely and by a untrained personal it may lead to several short-term and long-term health problems, some of which are not reconcilable with life. Medical disadvantages of FGC can be classified into two groups, which involve early and long-term complications:
Early complications:
- Acute pain
- Shock
- Hemorrhage
- Tetanus, necrosis, systemic or local infection with HIV, hepatitis B and C, and other viruses
- Inability to urinate.
- Damage/injury to neighbouring organs such as urethra, Bartholin duct or skene Glans.
- Death
Long-term complications:
- Chronic vaginal or lower abdominal infections
- Menstrual irregularities, painful menstruation, obstruction of menstrual flow
- Difficulty with urination and persistent urinary tract infections
- Urinary incontinence
- Injuries to the reproductive system and infertility
- Abscess, scars, and cyst formation.
- Labour and delivery complications and neonatal deaths
- Painful and unpleasant sexual intercourse
- Psychological trauma, loss of motivation, anxiety, and depression
The above complications are type related. Type 1A don’t lead to any of these complications and type one as a whole has only limited complications. A medical perspective on female genital cutting especially type 2 and type 3 paints a more devastating picture with regard to sexual health and happiness. The labia minora and majora (are the parts of the genitalia that are mutilated by type 2 and type 3), the clitoris are covered by rich neural networks and are sensitive to sexual stimulation. Sexual stimulation and pleasure increase vaginal secretion, preparing the woman and thus, the man, for a comfortable sexual intercourse. Loss of such sensitive organs may result in vaginal dryness if other sensitive areas aren’t stimulated or there is no adequate foreplay making it more difficult to have pleasure and orgasm. In case of repetition, this gradually evolves into sexual frigidity and unhappiness. It leads to sexual dysfunction, first in the woman and later in man. Narrowing of the vaginal opening as performed in certain types 3 causes pain and hemorrhage during penile penetration in sexual intercourse. It may lead to prolong labour and consequent caesarean section. If delivery happens the exposed area may lead to excessive bleeding. It is believe that narrowing of vaginal opening (‘sealing’) is done to maintain virginity by hindering premarital sex hence maintaining chastity. In children type 2 and type 3 can lead too urine retention and cryptomenorrhea as well as injury to adjacent organs.
However, there is an exception to complications of female genital cutting, called hoodectomy or clitoral hood reduction as well as labial reduction surgery and with or without clitoridectomy. Hoodectomy without clitoridectomy is what islam scholars says is the Prophet advice is Sunnah. This procedure deserves additional explanation.
The hood (Prepuce) is a fold of skin surrounding the glans penis in men and the clitoris in women. It is the part that is removed in male circumcision. In some girls, this fold of skin is redundant or overdevelops during puberty, thus covering the clitoris entirely and preventing sufficient contact between the penis and the clitoris during sexual intercourse as well as causing discomfort for woman because of squeezing under the pressure of male external genitalia. The clitoris can also enlarge. There can also be accumulation of SMEGMA (combination of secretions, discharges debris and dead cells) that can accumulate under the hood leading to risk of Sexual transmitted infections, inflammations, adhesions and pain. This results in a loss of stimulation, preventing the woman from having pleasure and orgasm. Removal of such redundant folds of skin through hoodectomy (clitoral hood reduction) increases pleasure during intercourse and facilitates orgasm. The presence of such redundant skin is a real medical indication for surgery, and its removal is beneficial to sexual health. Today, clitoral hood reduction and similar types of hoodoplasty with or without cllitoridectomy are among the most common aesthetic genital surgeries in the western countries.
In a 1979 report, WHO underlined the fact that this type of surgical intervention does not present any harm. “With regard to the type of FC which involves removal of the prepuce of the clitoris, which is similar to male circumcision, no harmful health effects have been noted.” Thabet and Thabet have also showed that individuals who underwent type-1A Female Circumcision (hoodectomy only) is not different from uncircumcised women in terms of sexual scores obtained from both groups.
Amendment of act No 12 of 2010
32A: prohibition of female circumcision
1: a person shall not engage in female circumcision
2: a person who engage in female circumcision commits an offense and is liable on conviction
- To imprisonment for a term of three years or a fine of fifty thousand dalasis or to both and
- Where female circumcision cause death to life imprisonment
3: Female circumcision includes
- The excision of prepuce with partial or total excision of clitoris (clitoridectomy)
- The Partial or total excision of labia minora
- The Partial or total excision of external genitalia (of the labia minora and labia majora) including stitching.
- The stitching with thorns straws threads or by other means in order to connect the excision of labia and the cutting of the vagina and introduction of corrosive substances or herbs in the vagina for the purpose of narrowing it
- Symbolic practice that involves nicking and pricking of the clitoris to release drop of blood: or
- Engaging in any form of female genital mutilation or cutting
32B accomplice to female circumcision
- A person who requests incite or promote female circumcision by providing tools or by any other means commits an offense and is liable on conviction to imprisonment for a term of three years or a fine of fifty thousand dalasis or both
- A person who knows female circumcision is about to take place or has taken place and fails, without good cause, to warn or inform, as the case may be, the proper authorities promptly, commits an offense and is liable on conviction to a fine of ten thousand dalasis.
Medical concerns of the law to health personals
1: The law definition of female circumcision 32A3. doesn’t exempt those procedures that are as a result of medical indication hence a medical personal who perform surgery on a person may be liability eg hoodectomy as results of excessive tissue or clitoridectomy as result excessive enlarge clitoris like clitorimegaly as in those with ambiguous genitalia.
There needs to be a distinction between female circumcision for traditional, religious or cosmetic purpose and medical treatment indication.
The law has blanked ban even for adults who have reach age of consent aren’t allow to determine for themselves how they desire their genital appears. Especially if its aesthetic or medical reason. Those adults with redundant labia and enlarge clitoris will continue to experience discomfort with persistent friction leading to bruises and unsolicited sexual stimulation by their clothing’s or thighs. This can have lots of psychological impact on them as it will hinder their social engagements
2: accomplish penalty
Medical personnel who examined girls who underwent female circumcision. The law is compelling them to report it or face penalty ie 32B2/ it might compromise patient provider confidentiality which may greatly affect trust in the already existing huge mistrust between clients and health care providers in the Gambia.
There should be modification of the law to exempt health care workers to maintain client health care provider confidentiality so that clients wont default from their health care.
3: OBGYN Practice: has both medical and surgical components. A part of the surgical component involves procedures on the vulva and vagina. These procedures may include nicking, pricking, cutting, excision, stitching etc. Urologist and paediatrist surgeons too might be affected.
The law doesn’t discriminate medical intervention and circumcision hence some medical interventions will be illegal consequently risk prosecution.
32A subsection a – d will mean any procedure on the vulva by a doctor can be term circumcision and the medical personnel can be accused of breaking the law by performing FGM
Episiotomy is the commonest procedure to perform during labour and delivery involves cutting then stitching. This is considered by this law as circumcision hence doctors and midwives may be criminal liable.
Marsupialization, vulvectomy, Hymenectomy, vaginoplasty etc all involves cutting stitching etc hence performing circumcision as per the law.
4: Aesthetic Surgery
Hoodectomy, Virginity restoration surgery or vulvectomy, vulvoplasty (in causes of malignancies) and adult patients request are an offence in this law. Aesthetic surgery is new branch of plastic surgery which our country is lacking far behind.
The issue of prove of virginity on first night for newly married young women are still a cause of psychological concerns. Clients regularly visit our clinic seeking help/assistance with virginity restoration so that the shame on them and their family will be avoided. This too is a gender-based violence which our women go through which requires advocacy.
Illegalisation and its consequences
Illegalisation may lead to unsafe and unregulated practice which will increase morbidity and mortality just like the experiences of criminalisation of abortion which we see on a regular basis. We urge a revisit of the law and possible medicalisation with registration and licenses of practitioners.
Psychological trauma to those who believe it a religious obligation or a traditional requirement. WHO define health as psychological well being. One cannot feel well if they believe they have an ailment that need removal hence with the ban in place we may be face with lots of clients with psychological trauma. Mental health deny is denying individuals fundamental human right because health is a fundamental right. This includes those with enlarge prepuce clitoris and labia who be denied treatment.
Criminalising the practice may lead to creating a lot of the victims in social centres which will be an extra burden to GOTG. as the parents or guidance’s will be consider perpetrators/accomplices by the law and may face prosecution and conviction. I believe the practitioners should be the only person made liable as it happens in medical practice to practitioners. The parents and guidance should be considered as victims
In medicine practice there is a saying ‘don make the cure worse than the disease’
If I may quote Trump: ‘we can’t let the cure worse than the disease’
RECOMMENDATIONS AMENDMENT THE LAW
1: To exclude medical procedures that requires cut to the external genitalia
2: To exclude health care workers as accomplish if they examine client but doesn’t report it
3: To exclude victim and their parents/guidance as perpetrators and or accomplishes to avoid them defaulting medical care
4: Ban female genital mutilation type 2, type 3 and type 4
5: legalise Type 1A and trained practitioners who should be medical practitioners and licenses to provide female circumcision type 1 in a medical facility under sterile conditions.
6: traditional and religious leaders support Ministry of Health in advocacy against type 2, type 3 and type 4 as well as prove of virginity. Classifying them as gender Base Violence
7: to prosecute those unlicensed circumcisers or anyone who performed type 2.3 or 4 FGM
Musa Marena
Medical Practitioner


